Infective endocarditis is a severe infection that affects the inner lining of the heart chambers and valves, posing a significant risk to the cardiovascular system. The condition is primarily instigated by bacteria entering the bloodstream and adhering to damaged areas of the heart, particularly heart valves. Those with pre-existing heart conditions, congenital heart defects, prosthetic heart valves, or a history of intravenous drug use are at an elevated risk. Common bacterial culprits include species from Streptococcus and Staphylococcus.
Clinical presentation of infective endocarditis involves a range of symptoms, including fever, fatigue, weight loss, and night sweats. As the infection progresses, cardiovascular symptoms may emerge, such as new or changing heart murmurs, chest pain, and shortness of breath. The diverse array of symptoms can lead to challenges in diagnosis, with some cases exhibiting subtle manifestations that delay recognition.
Diagnosis relies on a combination of clinical evaluation, blood tests, and imaging studies. Blood cultures are pivotal in identifying the causative bacteria, while echocardiography (transthoracic or transesophageal) provides detailed images of the heart valves and chambers, aiding in the detection of vegetations or masses indicative of infection.
Management of infective endocarditis involves a multidisciplinary approach, often with input from infectious disease specialists and cardiologists. Antibiotic therapy is a fundamental component, tailored to the identified causative bacteria. Surgical intervention may be necessary in certain cases to repair or replace damaged heart valves, drain abscesses, or remove infected tissues.
Complications of infective endocarditis can be severe, including heart failure, embolism, and abscess formation. Prognosis varies based on factors like the timeliness of diagnosis, the specific bacteria involved, and underlying heart conditions. While many individuals can recover with prompt and appropriate treatment, the condition requires meticulous management to prevent recurrence and mitigate potential complications. Infective endocarditis underscores the intricate relationship between cardiovascular health and infectious diseases, emphasizing the importance of vigilant monitoring in individuals with predisposing factors.
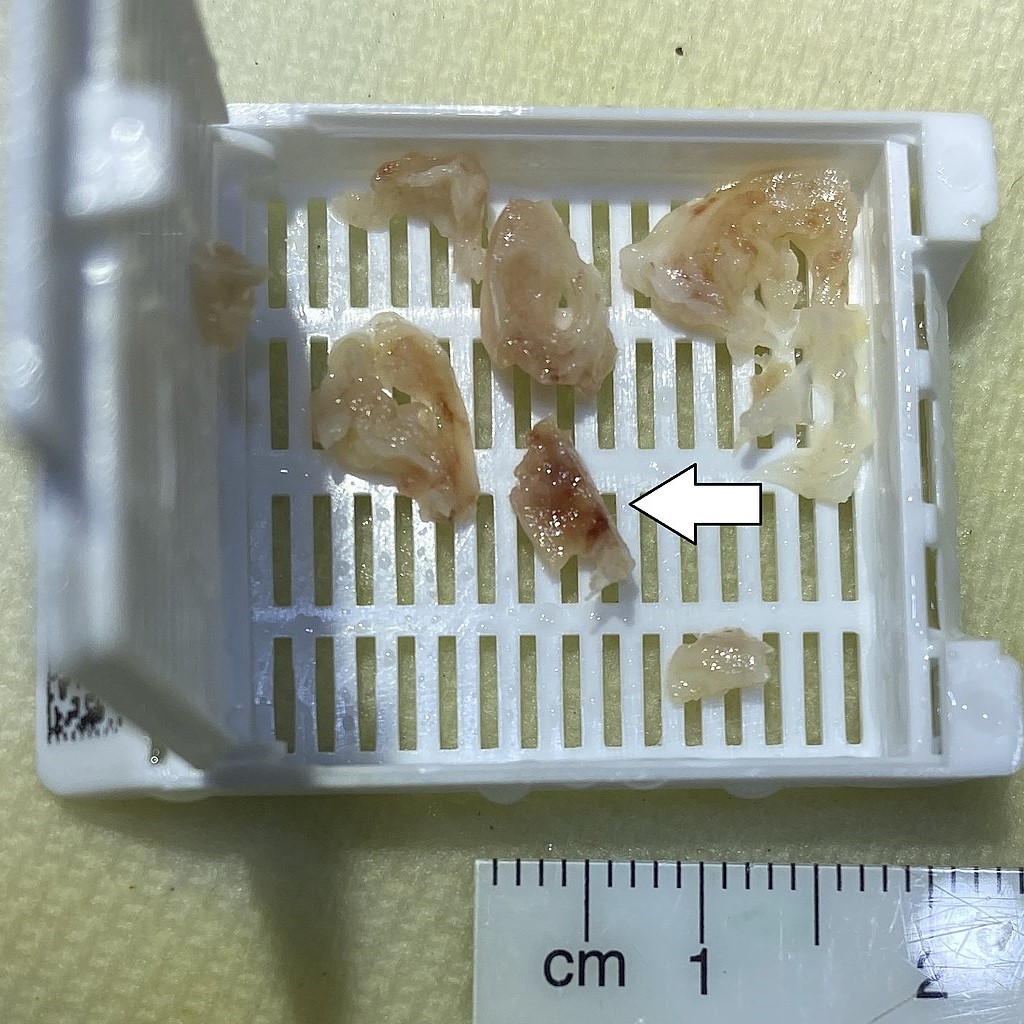
Gross pathology of vegetation of infective endocarditis
Do you want to know more about Infective endocarditis? Let’s take a look at these 28 interesting facts about infective endocarditis?
- Rare but Serious: Infective endocarditis is a relatively rare condition but is considered a serious and potentially life-threatening infection of the heart.
- Valve Affection: The infection often affects heart valves, causing inflammation and damage.
- Bacterial Culprits: Common bacteria causing infective endocarditis include Streptococcus and Staphylococcus species. However, a variety of other bacteria and fungi can also be responsible.
- Risk Factors: Predisposing factors include pre-existing heart conditions, congenital heart defects, prosthetic heart valves, and a history of intravenous drug use.
- Bloodstream Invasion: The condition typically arises when bacteria enter the bloodstream and adhere to damaged areas of the heart.
- Challenging Diagnosis: Diagnosis can be challenging due to a diverse range of symptoms, including fever, fatigue, weight loss, and cardiovascular symptoms like chest pain and shortness of breath.
- Echocardiography Importance: Echocardiography, both transthoracic and transesophageal, is crucial for diagnosing infective endocarditis by revealing vegetations or masses on heart valves.
- Blood Culture Identification: Blood cultures are essential for identifying the specific bacteria causing the infection, guiding antibiotic treatment.
- Dental Procedures Connection: Dental procedures, especially those involving manipulation of the gums or oral tissues, can sometimes introduce bacteria into the bloodstream, posing a potential risk for infective endocarditis.
- Prevention Measures: Antibiotic prophylaxis before certain dental procedures was once recommended to prevent infective endocarditis in individuals at risk, but guidelines have evolved, and the practice is more restricted today.
- Complications Abound: Infective endocarditis can lead to various complications, including heart failure, embolism, abscess formation, and damage to other organs.
- Surgical Intervention: In severe cases, surgical intervention may be necessary to repair or replace damaged heart valves and address complications.
- Vegetations and Infected Masses: Vegetations, composed of bacteria and blood clots, often form on heart valves and can embolize, traveling to other parts of the body.
- Subacute and Acute Forms: The condition can manifest in subacute or acute forms, with subacute cases having a more gradual onset and often milder symptoms.
- Community-Acquired and Healthcare-Associated: Infective endocarditis can be classified as community-acquired or healthcare-associated, depending on where the infection is acquired.
- Intravenous Drug Use Risk: Individuals who engage in intravenous drug use are at an increased risk of developing infective endocarditis due to the potential introduction of bacteria through contaminated needles.
- Immunological Response: The body’s immune response to the infection can lead to the formation of small, painful nodules on the fingertips known as Osler’s nodes.
- Janeway Lesions: Janeway lesions are non-tender, red or purple spots that may appear on the palms or soles due to small hemorrhages.
- Roth Spots: Roth spots are retinal hemorrhages with a white or pale center that can be seen on eye examination.
- Spleen Enlargement: Infective endocarditis can cause enlargement of the spleen, contributing to abdominal discomfort.
- Chills and Sweating: Symptoms such as chills and excessive sweating, especially at night, can be indicative of infective endocarditis.
- Increased Risk with Aging: The risk of developing infective endocarditis increases with age, with a higher incidence in older individuals.
- Gender Disparity: Men are more commonly affected by infective endocarditis than women.
- Antibiotic Therapy Challenges: Treatment involves prolonged courses of intravenous antibiotics, often administered in a hospital setting, posing challenges for outpatient management.
- Mortality Rates: Mortality rates for infective endocarditis vary but can be significant, particularly in cases with delayed diagnosis or complications.
- Association with Rheumatic Fever: In some cases, infective endocarditis can be associated with previous episodes of rheumatic fever, especially in regions where rheumatic heart disease is prevalent.
- Chronic Valve Damage: Even with successful treatment, infective endocarditis can lead to chronic valve damage, necessitating ongoing monitoring.
- Interdisciplinary Care: Managing infective endocarditis often requires an interdisciplinary approach involving cardiologists, infectious disease specialists, and sometimes cardiovascular surgeons.
Infective endocarditis, with its intricate dance between bacterial invasion and the delicate structures of the heart, represents a formidable challenge in the realm of cardiovascular health. From the subtle, elusive symptoms to the potential life-threatening complications, this condition underscores the critical need for vigilance, early diagnosis, and comprehensive management. As medical science continues to delve into the complexities of infective endocarditis, the importance of an interdisciplinary approach, involving cardiologists, infectious disease specialists, and surgical experts, becomes increasingly evident. In the journey towards healing, the delicate balance between prompt antibiotic intervention and, in some cases, surgical correction navigates the intricate landscape of the heart’s vulnerabilities. The ongoing exploration of infective endocarditis serves as a testament to our ceaseless pursuit of understanding and addressing the challenges posed by infectious diseases in the realm of cardiovascular well-being.





